Renal function
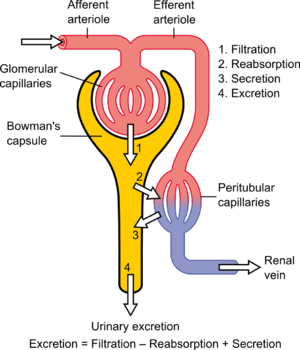
Diagram showing the basic physiologic mechanisms of the kidney
Renal function, in nephrology, is an indication of the kidney's condition and its role in renal physiology. Glomerular filtration rate (GFR) describes the flow rate of filtered fluid through the kidney. Creatinine clearance rate (CCr or CrCl) is the volume of blood plasma that is cleared of creatinine per unit time and is a useful measure for approximating the GFR. Creatinine clearance exceeds GFR due to creatinine secretion,[citation needed] which can be blocked by cimetidine. In alternative fashion, overestimation by older serum creatinine methods resulted in an underestimation of creatinine clearance, which provided a less biased estimate of GFR.[1] Both GFR and CCr may be accurately calculated by comparative measurements of substances in the blood and urine, or estimated by formulas using just a blood test result (eGFR and eCCr).
The results of these tests are used to assess the excretory function of the kidneys. Staging of chronic kidney disease is based on categories of GFR as well as albuminuria and cause of kidney disease.[2]
Dosage of drugs that are excreted primarily via urine may need to be modified based on either GFR or creatinine clearance.
Contents
1 Indirect markers
2 Glomerular filtration rate
2.1 Measurement using inulin
2.2 Measurement with radioactive tracers
2.3 Pressure definition
2.3.1 Kf
2.3.2 PG
2.3.3 PB
2.3.4 ∏G
2.3.5 ∏B
3 Creatinine-based approximations of GFR
3.1 Creatinine clearance CCr
4 Estimated values
4.1 Estimated creatinine clearance rate (eCCr) using Cockcroft-Gault formula
4.2 Estimated GFR (eGFR) using Modification of Diet in Renal Disease (MDRD) formula
4.3 Estimated GFR (eGFR) using the CKD-EPI formula
4.4 Estimated GFR (eGFR) using the Mayo Quadratic formula
4.5 Estimated GFR for children using Schwartz formula
4.6 Importance of calibration of the serum creatinine level and the IDMS standardization effort
4.7 Cystatin C
5 Normal ranges
6 Decreased renal function
6.1 Chronic kidney disease stages
7 See also
8 References
9 External links
9.1 Online calculators
9.2 Reference links
Indirect markers
Most doctors use the plasma concentrations of the waste substances of creatinine and urea (U), as well as electrolytes (E), to determine renal function. These measures are adequate to determine whether a patient is suffering from kidney disease.
However, blood urea nitrogen (BUN) and creatinine will not be raised above the normal range until 60% of total kidney function is lost. Hence, the more accurate Glomerular filtration rate or its approximation of the creatinine clearance is measured whenever renal disease is suspected or careful dosing of nephrotoxic drugs is required.
Elevated protein levels in urine mark some kidney disease. The most sensitive marker of proteinuria is elevated urine albumin. Persistent presence of more than 30 mg albumin per gram creatinine in the urine is diagnostic of chronic kidney disease (microalbuminuria is a level of 30 mg/L to 299 mg/L urine or 30–299 mg/24 h; a concentration of albumin in the urine that is not detected by usual urine dipstick methods).
Glomerular filtration rate
Glomerular filtration rate (GFR) is the volume of fluid filtered from the renal (kidney) glomerular capillaries into the Bowman's capsule per unit time.[3] Central to the physiologic maintenance of GFR is the differential basal tone of the afferent and efferent arterioles (see diagram). In other words, the filtration rate is dependent on the difference between the higher blood pressure created by vasoconstriction of the input or afferent arteriole versus the lower blood pressure created by lesser vasoconstriction of the output or efferent arteriole.
GFR is equal to the Clearance Rate when any solute is freely filtered and is neither reabsorbed nor secreted by the kidneys. The rate therefore measured is the quantity of the substance in the urine that originated from a calculable volume of blood. Relating this principle to the below equation – for the substance used, the product of urine concentration and urine flow equals the mass of substance excreted during the time that urine has been collected. This mass equals the mass filtered at the glomerulus as nothing is added or removed in the nephron. Dividing this mass by the plasma concentration gives the volume of plasma which the mass must have originally come from, and thus the volume of plasma fluid that has entered Bowman's capsule within the aforementioned period of time. The GFR is typically recorded in units of volume per time, e.g., milliliters per minute (mL/min). Compare to filtration fraction.
- GFR=Urine Concentration×Urine FlowPlasma Concentration{displaystyle GFR={frac {{mbox{Urine Concentration}}times {mbox{Urine Flow}}}{mbox{Plasma Concentration}}}}

There are several different techniques used to calculate or estimate the glomerular filtration rate (GFR or eGFR). The above formula only applies for GFR calculation when it is equal to the Clearance Rate.
Measurement using inulin
The GFR can be determined by injecting inulin or the inulin-analog sinistrin into the plasma. Since both inulin and sinistrin are neither reabsorbed nor secreted by the kidney after glomerular filtration, their rate of excretion is directly proportional to the rate of filtration of water and solutes across the glomerular filter. Compared to the MDRD formula[clarification needed], the inulin clearance slightly overestimates the glomerular function. In early stage renal disease, the inulin clearance may remain normal due to hyperfiltration in the remaining nephrons.[4] Incomplete urine collection is an important source of error in inulin clearance measurement.[5]
Measurement with radioactive tracers
GFR can be accurately measured using radioactive substances, in particular Chromium-51 and Technetium-99m. These come close to the ideal properties of Inulin (undergoing only glomerular filtration) but can be measured more practically with only a few urine or blood samples.[6] Measurement of renal or plasma clearance of 51Cr-EDTA is widely used in Europe but not available in the United States, where 99mTc-DTPA may be used instead.[7] Renal and plasma clearance 51Cr-EDTA has been shown to be accurate in comparison with the gold standard, Inulin.[8][9][10] Use of 51Cr‑EDTA is considered a reference standard measure in UK guidance.[11]
Pressure definition
More precisely, GFR is the fluid flow rate between the glomerular capillaries and the Bowman's capsule:
dQdt=Kf×(PG−PB−ΠG+ΠB){displaystyle {operatorname {d} Q over operatorname {d} t}=K_{f}times (P_{G}-P_{B}-Pi _{G}+Pi _{B})}[12][13]
Where:
dQdt{displaystyle {operatorname {d} Q over operatorname {d} t}}is the GFR.
Kf{displaystyle K_{f}}is called the filtration constant and is defined as the product of the hydraulic conductivity and the surface area of the glomerular capillaries.
PG{displaystyle P_{G}}is the hydrostatic pressure within the glomerular capillaries.
PB{displaystyle P_{B}}is the hydrostatic pressure within the Bowman's capsule.
ΠG{displaystyle Pi _{G}}is the colloid osmotic pressure within the glomerular capillaries.
- and ΠB{displaystyle Pi _{B}}
is the colloid osmotic pressure within the Bowman's capsule.
Kf
Because this constant is a measurement of hydraulic conductivity multiplied by the capillary surface area, it is almost impossible to measure physically. However, it can be determined experimentally. Methods of determining the GFR are listed in the above and below sections and it is clear from our equation that Kf{displaystyle K_{f}}
- Kf=GFRNet Filt. Pressure=GFR(PG−PB−ΠG+ΠB){displaystyle K_{f}={frac {textrm {GFR}}{text{Net Filt. Pressure}}}={frac {textrm {GFR}}{(P_{G}-P_{B}-Pi _{G}+Pi _{B})}}}

PG
The hydrostatic pressure within the glomerular capillaries is determined by the pressure difference between the fluid entering immediately from the afferent arteriole and leaving through the efferent arteriole. The pressure difference is approximated by the product of the total resistance of the respective arteriole and the flux of blood through it:[13]
- Pa−PG=Ra×Qa{displaystyle P_{a}-P_{G}=R_{a}times Q_{a}}

- PG−Pe=Re×Qe{displaystyle P_{G}-P_{e}=R_{e}times Q_{e}}

Where:
Pa{displaystyle P_{a}}is the afferent arteriole pressure.
PG{displaystyle P_{G}}
Pe{displaystyle P_{e}}is the efferent arteriole pressure.
Ra{displaystyle R_{a}}is the afferent arteriole resistance.
Re{displaystyle R_{e}}is the efferent arteriole resistance.
Qa{displaystyle Q_{a}}is the afferent arteriole flux.
- And, Qe{displaystyle Q_{e}}
is the efferent arteriole flux.
PB
The pressure in the Bowman's capsule and proximal tubule can be determined by the difference between the pressure in the Bowman's capsule and the descending tubule:[13]
- PB−Pd=Rd×(Qa−Qe){displaystyle P_{B}-P_{d}=R_{d}times (Q_{a}-Q_{e})}

Where:
Pd{displaystyle P_{d}}is the pressure in the descending tubule.
- And, Rd{displaystyle R_{d}}
is the resistance of the descending tubule.
∏G
Blood plasma has a good many proteins in it and they exert an inward directed force called the colloid osmotic pressure on the water in hypotonic solutions across a membrane, i.e., in the Bowman's capsule. Because plasma proteins are virtually incapable of escaping the glomerular capillaries, this oncotic pressure is defined, simply, by the ideal gas law:[12][13]
- ΠG=RTc{displaystyle Pi _{G}=RTc}

Where:
- R is the universal gas constant
- T is the temperature.
- And, c is concentration in mol/L of plasma proteins (remember the solutes can freely diffuse through the glomerular capsule).
∏B
This value is almost always taken to be equal to zero because, in a healthy nephron, there should be no proteins in the Bowman's Capsule.[12]
Creatinine-based approximations of GFR
In clinical practice, however, creatinine clearance or estimates of creatinine clearance based on the serum creatinine level are used to measure GFR. Creatinine is produced naturally by the body (creatinine is a breakdown product of creatine phosphate, which is found in muscle). It is freely filtered by the glomerulus, but also actively secreted by the peritubular capillaries in very small amounts such that creatinine clearance overestimates actual GFR by 10% to 20%. This margin of error is acceptable, considering the ease with which creatinine clearance is measured. Unlike precise GFR measurements involving constant infusions of inulin, creatinine is already at a steady-state concentration in the blood, and so measuring creatinine clearance is much less cumbersome. However, creatinine estimates of GFR have their limitations. All of the estimating equations depend on a prediction of the 24-hour creatinine excretion rate, which is a function of muscle mass which is quite variable. One of the equations, the Cockcroft and Gault equation (see below) does not correct for race. With a higher muscle mass, serum creatinine will be higher for any given rate of clearance.
A common mistake made when just looking at serum creatinine is the failure to account for muscle mass. Hence, an older woman with a serum creatinine of 1.4 mg/dL may actually have a moderately severe degree of renal insufficiency, whereas a young muscular male can have a normal level of renal function at this serum creatinine level. Creatinine-based equations should be used with caution in cachectic patients and patients with cirrhosis. They often have very low muscle mass and a much lower creatinine excretion rate than predicted by the equations below, such that a cirrhotic patient with a serum creatinine of 0.9 mg/dL may have a moderately severe degree of renal insufficiency.
Creatinine clearance CCr
One method of determining GFR from creatinine is to collect urine (usually for 24 h) to determine the amount of creatinine that was removed from the blood over a given time interval. If one removes 1440 mg in 24 h, this is equivalent to removing 1 mg/min. If the blood concentration is 0.01 mg/mL (1 mg/dL), then one can say that 100 mL/min of blood is being "cleared" of creatinine, since, to get 1 mg of creatinine, 100 mL of blood containing 0.01 mg/mL would need to have been cleared.
Creatinine clearance (CCr) is calculated from the creatinine concentration in the collected urine sample (UCr), urine flow rate (Vdt), and the plasma concentration (PCr). Since the product of urine concentration and urine flow rate yields creatinine excretion rate, which is the rate of removal from the blood, creatinine clearance is calculated as removal rate per min (UCr×Vdt) divided by the plasma creatinine concentration. This is commonly represented mathematically as
- CCr=UCr×V˙PCr{displaystyle C_{Cr}={frac {U_{Cr}times {dot {V}}}{P_{Cr}}}}

Example: A person has a plasma creatinine concentration of 0.01 mg/ml and in 1 hour produces 60ml of urine with a creatinine concentration of 1.25 mg/mL.
- CCr=1.25mg/mL×60mL60min0.01mg/mL=1.25mg/mL×1mL/min0.01mg/mL=1.25mg/min0.01mg/mL=125mL/min{displaystyle C_{Cr}={frac {mathrm {1.25mg/mLtimes {frac {60mL}{60min}}} }{mathrm {0.01mg/mL} }}={frac {mathrm {{1.25mg/mL}times {1mL/min}} }{mathrm {0.01mg/mL} }}={frac {mathrm {1.25mg/min} }{mathrm {0.01mg/mL} }}=mathrm {125mL/min} }

The common procedure involves undertaking a 24-hour urine collection, from empty-bladder one morning to the contents of the bladder the following morning, with a comparative blood test then taken. The urinary flow rate is still calculated per minute, hence:
- CCr=UCr × 24-hour volumePCr × 24×60min{displaystyle C_{Cr}={frac {U_{Cr} times {text{24-hour volume}}}{mathrm {P_{Cr} times 24times 60min} }}}

To allow comparison of results between people of different sizes, the CCr is often corrected for the body surface area (BSA) and expressed compared to the average sized man as mL/min/1.73 m2. While most adults have a BSA that approaches 1.7 m2 (1.6 m2 to 1.9 m2), extremely obese or slim patients should have their CCr corrected for their actual BSA.
- CCr-corrected=CCr × 1.73BSA{displaystyle C_{text{Cr-corrected}}={frac {{C_{Cr}} times {1.73}}{mathrm {BSA} }}}
- BSA can be calculated on the basis of weight and height.

Twenty-four-hour urine collection to assess creatinine clearance is no longer widely performed, due to difficulty in assuring complete specimen collection. To assess the adequacy of a complete collection, one always calculates the amount of creatinine excreted over a 24-hour period. This amount varies with muscle mass, and is higher in young people vs. old, in blacks vs. whites, and in men vs. women. An unexpectedly low or high 24-hour creatinine excretion rate voids the test. Nevertheless, in cases where estimates of creatinine clearance from serum creatinine are unreliable, creatinine clearance remains a useful test. These cases include "estimation of GFR in individuals with variation in dietary intake (vegetarian diet, creatine supplements) or muscle mass (amputation, malnutrition, muscle wasting), since these factors are not specifically taken into account in prediction equations."[14]
Estimated values
A number of formulae have been devised to estimate GFR or Ccr values on the basis of serum creatinine levels. Where not otherwise stated serum creatinine is assumed to be stated in mg/dL, not µmol/L—divide by 88.4 to convert from µmol/Lto mg/dL.
Estimated creatinine clearance rate (eCCr) using Cockcroft-Gault formula
A commonly used surrogate marker for estimate of creatinine clearance is the Cockcroft-Gault (CG) formula, which in turn estimates GFR in ml/min:[15] It is named after the scientists, the asthmologist Donald William Cockcroft (b. 1946) and the nephrologist Matthew Henry Gault (1925–2003), who first published the formula in 1976, and it employs serum creatinine measurements and a patient's weight to predict the creatinine clearance.[16][17]
The formula, as originally published, is:
- eCCr=(140−Age) × Mass (in kilograms) × [0.85 if Female]72 × [Serum Creatinine (in mg/dL)]{displaystyle eC_{Cr}={frac {mathrm {(140-Age)} times {text{Mass (in kilograms)}} times [{text{0.85 if Female}}]}{mathrm {72} times [{text{Serum Creatinine (in mg/dL)}}]}}}
- This formula expects weight to be measured in kilograms and creatinine to be measured in mg/dL, as is standard in the USA. The resulting value is multiplied by a constant of 0.85 if the patient is female. This formula is useful because the calculations are simple and can often be performed without the aid of a calculator.
![{displaystyle eC_{Cr}={frac {mathrm {(140-Age)} times {text{Mass (in kilograms)}} times [{text{0.85 if Female}}]}{mathrm {72} times [{text{Serum Creatinine (in mg/dL)}}]}}}](https://wikimedia.org/api/rest_v1/media/math/render/svg/55b9b6ae6978b4b7f8a56e9394be2760ca420cc2)
When serum creatinine is measured in µmol/L:
- eCCr=(140−Age) × Mass (in kilograms) × Constant[Serum Creatinine (in μmol/L)]{displaystyle eC_{Cr}={frac {mathrm {(140-Age)} times {text{Mass (in kilograms)}} times {text{Constant}}}{[{text{Serum Creatinine (in }}mu mathrm {mol/L)} ]}}}
- Where Constant is 7000123000000000000♠1.23 for men and 7000104000000000000♠1.04 for women.
![{displaystyle eC_{Cr}={frac {mathrm {(140-Age)} times {text{Mass (in kilograms)}} times {text{Constant}}}{[{text{Serum Creatinine (in }}mu mathrm {mol/L)} ]}}}](https://wikimedia.org/api/rest_v1/media/math/render/svg/39889eb768a83f3491fdb804da627cf08a93d5be)
One interesting feature of the Cockcroft and Gault equation is that it shows how dependent the estimation of CCr is based on age. The age term is (140 – age). This means that a 20-year-old person (140 – 20 = 120) will have twice the creatinine clearance as an 80-year-old (140 – 80 = 60) for the same level of serum creatinine. The C-G equation assumes that a woman will have a 15% lower creatinine clearance than a man at the same level of serum creatinine.
Estimated GFR (eGFR) using Modification of Diet in Renal Disease (MDRD) formula
The most recently advocated formula for calculating the GFR is the one that was developed by the Modification of Diet in Renal Disease Study Group.[18] Most laboratories in Australia,[19] and The United Kingdom now calculate and report the MDRD estimated GFR along with creatinine measurements and this forms the basis of chronic kidney disease.[20] The adoption of the automatic reporting of MDRD-eGFR has been widely criticised.[21][22][23]
The most commonly used formula is the "4-variable MDRD," which estimates GFR using four variables: serum creatinine, age, ethnicity, and gender.[24] The original MDRD used six variables with the additional variables being the blood urea nitrogen and albumin levels.[18] The equations have been validated in patients with chronic kidney disease; however, both versions underestimate the GFR in healthy patients with GFRs over 60 mL/min.[25][26] The equations have not been validated in acute renal failure.
For creatinine in µmol/L:
- eGFR=32788 × [Serum Creatinine]−1.154 × Age−0.203 ×[1.212 if Black] ×[0.742 if Female]{displaystyle {text{eGFR}}={text{32788}} times [{text{Serum Creatinine}}]^{-1.154} times {text{Age}}^{-0.203} times {text{[1.212 if Black]}} times {text{[0.742 if Female]}}}
![{displaystyle {text{eGFR}}={text{32788}} times [{text{Serum Creatinine}}]^{-1.154} times {text{Age}}^{-0.203} times {text{[1.212 if Black]}} times {text{[0.742 if Female]}}}](https://wikimedia.org/api/rest_v1/media/math/render/svg/76bbf292dff353acdd0265df89f8595cc1db2dca)
For creatinine in mg/dL:
- eGFR=186 × [Serum Creatinine]−1.154 × Age−0.203 ×[1.212 if Black] ×[0.742 if Female]{displaystyle {text{eGFR}}={text{186}} times [{text{Serum Creatinine}}]^{-1.154} times {text{Age}}^{-0.203} times {text{[1.212 if Black]}} times {text{[0.742 if Female]}}}
- Creatinine levels in µmol/L can be converted to mg/dL by dividing them by 88.4. The 32788 number above is equal to 186×88.41.154.
![{displaystyle {text{eGFR}}={text{186}} times [{text{Serum Creatinine}}]^{-1.154} times {text{Age}}^{-0.203} times {text{[1.212 if Black]}} times {text{[0.742 if Female]}}}](https://wikimedia.org/api/rest_v1/media/math/render/svg/8f1326f39025418162a4205fce7f3c8b86fb66f6)
A more elaborate version of the MDRD equation also includes serum albumin and blood urea nitrogen (BUN) levels:
- eGFR=170 × [Serum Creatinine]−0.999 × Age−0.176 ×[0.762 if Female] ×[1.180 if Black] × BUN−0.170 × Albumin+0.318{displaystyle {text{eGFR}}={text{170}} times [{text{Serum Creatinine}}]^{-0.999} times {text{Age}}^{-0.176} times {text{[0.762 if Female]}} times {text{[1.180 if Black]}} times {text{BUN}}^{-0.170} times {text{Albumin}}^{+0.318}}
- where the creatinine and blood urea nitrogen concentrations are both in mg/dL. The albumin concentration is in g/dL.
![{displaystyle {text{eGFR}}={text{170}} times [{text{Serum Creatinine}}]^{-0.999} times {text{Age}}^{-0.176} times {text{[0.762 if Female]}} times {text{[1.180 if Black]}} times {text{BUN}}^{-0.170} times {text{Albumin}}^{+0.318}}](https://wikimedia.org/api/rest_v1/media/math/render/svg/9748d22c1c0a59f07eeb0d99047ffb992709043d)
These MDRD equations are to be used only if the laboratory has NOT calibrated its serum creatinine measurements to isotope dilution mass spectrometry (IDMS). When IDMS-calibrated serum creatinine is used (which is about 6% lower), the above equations should be multiplied by 175/186 or by 0.94086.[27]
Since these formulae do not adjust for body mass, they (relative to the Cockcroft-Gault formula) underestimate eGFR for heavy people and overestimate it for underweight people. (see Cockcroft-Gault formula above).
Estimated GFR (eGFR) using the CKD-EPI formula
The CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration) formula was published in May 2009. It was developed in an effort to create a formula more accurate than the MDRD formula, especially when actual GFR is greater than 60 mL/min per 1.73 m2.
Researchers pooled data from multiple studies to develop and validate this new equation. They used 10 studies that included 8254 participants, randomly using 2/3 of the data sets for development and the other 1/3 for internal validation. Sixteen additional studies, which included 3896 participants, were used for external validation.
The CKD-EPI equation performed better than the MDRD (Modification of Diet in Renal Disease Study) equation, especially at higher GFR, with less bias and greater accuracy. When looking at NHANES (National Health and Nutrition Examination Survey) data, the median estimated GFR was 94.5 mL/min per 1.73 m2 vs. 85.0 mL/min per 1.73 m2, and the prevalence of chronic kidney disease was 11.5% versus 13.1%. Despite its overall superiority to the MDRD equation, the CKD-EPI equations performed poorly in certain populations, including black women, the elderly and the obese, and was less popular among clinicians than the MDRD estimate.[28]
The CKD-EPI equation is:
- eGFR=141 × min(SCr/k,1)a × max(SCr/k,1)−1.209 × 0.993Age ×[1.018 if Female] ×[1.159 if Black] {displaystyle mathrm {eGFR} =141 times mathrm {min(SCr/k,1)} ^{a} times mathrm {max(SCr/k,1)} ^{-1.209} times 0.993^{text{Age}} times {text{[1.018 if Female]}} times {text{[1.159 if Black]}} }
![{displaystyle mathrm {eGFR} =141 times mathrm {min(SCr/k,1)} ^{a} times mathrm {max(SCr/k,1)} ^{-1.209} times 0.993^{text{Age}} times {text{[1.018 if Female]}} times {text{[1.159 if Black]}} }](https://wikimedia.org/api/rest_v1/media/math/render/svg/e695776a5827ef76b340344758106f09888735e6)
where SCr is serum creatinine (mg/dL), k is 0.7 for females and 0.9 for males, a is −0.329 for females and −0.411 for males, min indicates the minimum of SCr/k or 1, and max indicates the maximum of SCr/k or 1.
As separate equations for different populations:
For creatinine (IDMS calibrated) in mg/dL:
- Black female
- If serum creatinine (Scr) ≤ 0.7
- eGFR=166 × (SCr/0.7)−0.329 × 0.993Age {displaystyle mathrm {eGFR} =166 times mathrm {(SCr/0.7)} ^{-0.329} times 0.993^{text{Age}} }
- eGFR=166 × (SCr/0.7)−0.329 × 0.993Age {displaystyle mathrm {eGFR} =166 times mathrm {(SCr/0.7)} ^{-0.329} times 0.993^{text{Age}} }
- If serum creatinine (Scr) > 0.7
- eGFR=166 × (SCr/0.7)−1.209 × 0.993Age {displaystyle mathrm {eGFR} =166 times mathrm {(SCr/0.7)} ^{-1.209} times 0.993^{text{Age}} }
- eGFR=166 × (SCr/0.7)−1.209 × 0.993Age {displaystyle mathrm {eGFR} =166 times mathrm {(SCr/0.7)} ^{-1.209} times 0.993^{text{Age}} }


- Black male
- If serum creatinine (Scr) ≤ 0.9
- eGFR=163 × (SCr/0.9)−0.411 × 0.993Age {displaystyle mathrm {eGFR} =163 times mathrm {(SCr/0.9)} ^{-0.411} times 0.993^{text{Age}} }
- eGFR=163 × (SCr/0.9)−0.411 × 0.993Age {displaystyle mathrm {eGFR} =163 times mathrm {(SCr/0.9)} ^{-0.411} times 0.993^{text{Age}} }
- If serum creatinine (Scr) > 0.9
- eGFR=163 × (SCr/0.9)−1.209 × 0.993Age {displaystyle mathrm {eGFR} =163 times mathrm {(SCr/0.9)} ^{-1.209} times 0.993^{text{Age}} }
- eGFR=163 × (SCr/0.9)−1.209 × 0.993Age {displaystyle mathrm {eGFR} =163 times mathrm {(SCr/0.9)} ^{-1.209} times 0.993^{text{Age}} }


- Female, not black
- If serum creatinine (Scr) ≤ 0.7
- eGFR=144 × (SCr/0.7)−0.329 × 0.993Age {displaystyle mathrm {eGFR} =144 times mathrm {(SCr/0.7)} ^{-0.329} times 0.993^{text{Age}} }
- eGFR=144 × (SCr/0.7)−0.329 × 0.993Age {displaystyle mathrm {eGFR} =144 times mathrm {(SCr/0.7)} ^{-0.329} times 0.993^{text{Age}} }
- If serum creatinine (Scr) > 0.7
- eGFR=144 × (SCr/0.7)−1.209 × 0.993Age {displaystyle mathrm {eGFR} =144 times mathrm {(SCr/0.7)} ^{-1.209} times 0.993^{text{Age}} }
- eGFR=144 × (SCr/0.7)−1.209 × 0.993Age {displaystyle mathrm {eGFR} =144 times mathrm {(SCr/0.7)} ^{-1.209} times 0.993^{text{Age}} }


- Male, not black
- If serum creatinine (Scr) ≤ 0.9
- eGFR=141 × (SCr/0.9)−0.411 × 0.993Age {displaystyle mathrm {eGFR} =141 times mathrm {(SCr/0.9)} ^{-0.411} times 0.993^{text{Age}} }
- eGFR=141 × (SCr/0.9)−0.411 × 0.993Age {displaystyle mathrm {eGFR} =141 times mathrm {(SCr/0.9)} ^{-0.411} times 0.993^{text{Age}} }
- If serum creatinine (Scr) > 0.9
- eGFR=141 × (SCr/0.9)−1.209 × 0.993Age {displaystyle mathrm {eGFR} =141 times mathrm {(SCr/0.9)} ^{-1.209} times 0.993^{text{Age}} }
- eGFR=141 × (SCr/0.9)−1.209 × 0.993Age {displaystyle mathrm {eGFR} =141 times mathrm {(SCr/0.9)} ^{-1.209} times 0.993^{text{Age}} }


This formula was developed by Levey et al.[29]
The formula CKD-EPI may provide improved cardiovascular risk prediction over the MDRD Study formula in a middle-age population.[30]
Estimated GFR (eGFR) using the Mayo Quadratic formula
Another estimation tool to calculate GFR is the Mayo Quadratic formula. This formula was developed by Rule et al.,[25] in an attempt to better estimate GFR in patients with preserved kidney function. It is well recognized that the MDRD formula tends to underestimate GFR in patients with preserved kidney function. Studies in 2008 found that the Mayo Clinic Quadratic Equation compared moderately well with radionuclide GFR, but had inferior bias and accuracy than the MDRD equation in a clinical setting.[31][32]
The equation is:
eGFR=exp(1.911+5.249/[Serum Creatinine]−2.114/[Serum Creatinine]2−0.00686 × Age−[0.205 if Female]){displaystyle {text{eGFR}}={text{exp}}{(1.911+5.249/[{text{Serum Creatinine}}]-2.114/[{text{Serum Creatinine}}]^{2}-0.00686 times {text{Age}}-{text{[0.205 if Female]}})}}[32]
If Serum Creatinine < 0.8 mg/dL, use 0.8 mg/dL for Serum Creatinine.
Estimated GFR for children using Schwartz formula
In children, the Schwartz formula is used.[33][34] This employs the serum creatinine (mg/dL), the child's height (cm) and a constant to estimate the glomerular filtration rate:
- eGFR=k×HeightSerum Creatinine{displaystyle {text{eGFR}}={frac {{k}times {text{Height}}}{text{Serum Creatinine}}}}
- Where k is a constant that depends on muscle mass, which itself varies with a child's age:
- In first year of life, for pre-term babies k=0.33[35] and for full-term infants k=0.45[34]
- For infants and children of age 1 to 12 years, k=0.55.[33]
- In first year of life, for pre-term babies k=0.33[35] and for full-term infants k=0.45[34]

The method of selection of the constant k has been questioned as being dependent upon the gold-standard of renal function used (i.e. inulin clearance, creatinine clearance, etc.) and also may be dependent upon the urinary flow rate at the time of measurement.[36]
In 2009 the formula was updated to use standardized serum creatinine (recommend k=0.413) and additional formulas that allow improved precision were derived if serum cystatin C is measured in addition to serum creatinine.[37]
Importance of calibration of the serum creatinine level and the IDMS standardization effort
One problem with any creatinine-based equation for GFR is that the methods used to assay creatinine in the blood differ widely in their susceptibility to non-specific chromogens, which cause the creatinine value to be overestimated. In particular, the MDRD equation was derived using serum creatinine measurements that had this problem. The NKDEP program in the United States has attempted to solve this problem by trying to get all laboratories to calibrate their measures of creatinine to a "gold standard", which in this case is isotope dilution mass spectrometry (IDMS). In late 2009 not all labs in the U.S. had changed over to the new system. There are two forms of the MDRD equation that are available, depending on whether or not creatinine was measured by an IDMS-calibrated assay. The CKD-EPI equation is designed to be used with IDMS-calibrated serum creatinine values only.
Cystatin C
Problems with creatinine (varying muscle mass, recent meat ingestion (much less dependent on the diet than urea), etc.) have led to evaluation of alternative agents for estimation of GFR. One of these is cystatin C, a ubiquitous protein secreted by most cells in the body (it is an inhibitor of cysteine protease).
Cystatin C is freely filtered at the glomerulus. After filtration, Cystatin C is reabsorbed and catabolized by the tubular epithelial cells, with only small amounts excreted in the urine. Cystatin C levels are therefore measured not in the urine, but in the bloodstream.
Equations have been developed linking estimated GFR to serum cystatin C levels. Most recently, some proposed equations have combined (sex, age and race) adjusted cystatin C and creatinine. The most accurate is (sex, age and race) adjusted cystatin C, followed by (sex, age and race) adjusted creatinine and then cystatine C alone in slightly different with adjusted creatinine.[38]
Normal ranges
The normal range of GFR, adjusted for body surface area, is 100–130 average 125 mL/min/1.73m2 in men and 90–120 ml/min/1.73m2 in women younger than the age of 40. In children, GFR measured by inulin clearance is 110 mL/min/1.73 m2 until 2 years of age in both sexes, and then it progressively decreases. After age 40, GFR decreases progressively with age, by 0.4–1.2 mL/min per year.[citation needed]
Decreased renal function
A decreased renal function can be caused by many types of kidney disease. Upon presentation of decreased renal function, it is recommended to perform a history and physical examination, as well as performing a renal ultrasound and a urinalysis.[39] The most relevant items in the history are medications, edema, nocturia, gross hematuria, family history of kidney disease, diabetes and polyuria. The most important items in a physical examination are signs of vasculitis, lupus erythematosus, diabetes, endocarditis and hypertension.[39]
A urinalysis is helpful even when not showing any pathology, as this finding suggests an extrarenal etiology. Proteinuria and/or urinary sediment usually indicates the presence of glomerular disease. Hematuria may be caused by glomerular disease or by a disease along the urinary tract.[39]
The most relevant assessments in a renal ultrasound are renal sizes, echogenicity and any signs of hydronephrosis. Renal enlargement usually indicates diabetic nephropathy, focal segmental glomerular sclerosis or myeloma. Renal atrophy suggests longstanding chronic renal disease.[39]
Chronic kidney disease stages
Risk factors for kidney disease include diabetes, high blood pressure, family history, older age, ethnic group and smoking.
For most patients, a GFR over 60 mL/min/1.73m2 is adequate. But significant decline of the GFR from a previous test result can be an early indicator of kidney disease requiring medical intervention. The sooner kidney dysfunction is diagnosed and treated the greater odds of preserving remaining nephrons, and preventing the need for dialysis.
| CKD stage | GFR level (mL/min/1.73 m2) |
|---|---|
| Stage 1 | ≥ 90 |
| Stage 2 | 60–89 |
| Stage 3 | 30–59 |
| Stage 4 | 15–29 |
| Stage 5 | < 15 |
The severity of chronic kidney disease (CKD) is described by six stages; the most severe three are defined by the MDRD-eGFR value, and first three also depend on whether there is other evidence of kidney disease (e.g., proteinuria):
- 0) Normal kidney function – GFR above 90 mL/min/1.73 m2 and no proteinuria
- 1) CKD1 – GFR above 90 mL/min/1.73 m2 with evidence of kidney damage
- 2) CKD2 (mild) – GFR of 60 to 89 mL/min/1.73 m2 with evidence of kidney damage
- 3) CKD3 (moderate) – GFR of 30 to 59 mL/min/1.73 m2
- 4) CKD4 (severe) – GFR of 15 to 29 mL/min/1.73 m2
- 5) CKD5 kidney failure – GFR less than 15 mL/min/1.73 m2 Some people add CKD5D for those stage 5 patients requiring dialysis; many patients in CKD5 are not yet on dialysis.
Note: others add a "T" to patients who have had a transplant regardless of stage.
Not all clinicians agree with the above classification, suggesting that it may mislabel patients with mildly reduced kidney function, especially the elderly, as having a disease.[40][41] A conference was held in 2009 regarding these controversies by Kidney Disease: Improving Global Outcomes (KDIGO) on CKD: Definition, Classification and Prognosis, gathering data on CKD prognosis to refine the definition and staging of CKD.[42]
See also
- Clearance
- Dialysis
- Filtration fraction
- Kt/V
- Pharmacokinetics
- Renal clearance ratio
- Renal failure
- Standardized Kt/V
- Tubuloglomerular feedback
- Urea reduction ratio
References
^ Stevens LA, Coresh J, Greene T, Levey AS (June 2006). "Assessing kidney function—measured and estimated glomerular filtration rate". The New England Journal of Medicine. 354 (23): 2473–83. doi:10.1056/NEJMra054415. PMID 16760447..mw-parser-output cite.citation{font-style:inherit}.mw-parser-output q{quotes:"""""""'""'"}.mw-parser-output code.cs1-code{color:inherit;background:inherit;border:inherit;padding:inherit}.mw-parser-output .cs1-lock-free a{background:url("//upload.wikimedia.org/wikipedia/commons/thumb/6/65/Lock-green.svg/9px-Lock-green.svg.png")no-repeat;background-position:right .1em center}.mw-parser-output .cs1-lock-limited a,.mw-parser-output .cs1-lock-registration a{background:url("//upload.wikimedia.org/wikipedia/commons/thumb/d/d6/Lock-gray-alt-2.svg/9px-Lock-gray-alt-2.svg.png")no-repeat;background-position:right .1em center}.mw-parser-output .cs1-lock-subscription a{background:url("//upload.wikimedia.org/wikipedia/commons/thumb/a/aa/Lock-red-alt-2.svg/9px-Lock-red-alt-2.svg.png")no-repeat;background-position:right .1em center}.mw-parser-output .cs1-subscription,.mw-parser-output .cs1-registration{color:#555}.mw-parser-output .cs1-subscription span,.mw-parser-output .cs1-registration span{border-bottom:1px dotted;cursor:help}.mw-parser-output .cs1-hidden-error{display:none;font-size:100%}.mw-parser-output .cs1-visible-error{font-size:100%}.mw-parser-output .cs1-subscription,.mw-parser-output .cs1-registration,.mw-parser-output .cs1-format{font-size:95%}.mw-parser-output .cs1-kern-left,.mw-parser-output .cs1-kern-wl-left{padding-left:0.2em}.mw-parser-output .cs1-kern-right,.mw-parser-output .cs1-kern-wl-right{padding-right:0.2em}
^ Stevens, Paul E.; Levin, Adeera (Jun 4, 2013). "Evaluation and management of chronic kidney disease: synopsis of the kidney disease: improving global outcomes 2012 clinical practice guideline". Annals of Internal Medicine. 158 (11): 825–830. doi:10.7326/0003-4819-158-11-201306040-00007. ISSN 1539-3704. PMID 23732715.
^ Essentials of Human Physiology by Thomas M. Nosek. Section 7/7ch04/7ch04p11. – "Glomerular Filtration Rate"
^ GFR (Cockcroft & MDRD) calculator at medical-calculator.nl – Cockcroft-Gault and MDRD calculator and details about inulin clearance
^ Rose GA (1969). "Measurement of glomerular filtration rate by inulin clearance without urine collection". BMJ. 2: 91–3. doi:10.1136/bmj.2.5649.91.
^ Murray, A. W.; Barnfield, M. C.; Waller, M. L.; Telford, T.; Peters, A. M. (8 May 2013). "Assessment of Glomerular Filtration Rate Measurement with Plasma Sampling: A Technical Review". Journal of Nuclear Medicine Technology. 41 (2): 67–75. doi:10.2967/jnmt.113.121004.
^ Speeckaert, Marijn; Delanghe, Joris (2015). "Assessment of renal function". In Giuseppe, Daniel; Winearls, Christopher; Remuzzi, Giuseppe. Oxford Textbook of Clinical Nephrology (Fourth ed.). Oxford: Oxford University Press. p. 44. ISBN 9780199592548.
^ Henriksen, Ulrik L.; Henriksen, Jens H. (January 2015). "The clearance concept with special reference to determination of glomerular filtration rate in patients with fluid retention". Clinical Physiology and Functional Imaging. 35 (1): 7–16. doi:10.1111/cpf.12149.
^ Soveri, Inga; Berg, Ulla B.; Björk, Jonas; Elinder, Carl-Gustaf; Grubb, Anders; Mejare, Ingegerd; Sterner, Gunnar; Bäck, Sten-Erik (September 2014). "Measuring GFR: A Systematic Review". American Journal of Kidney Diseases. 64 (3): 411–424. doi:10.1053/j.ajkd.2014.04.010.
^ Hsu, C.-y.; Bansal, N. (22 July 2011). "Measured GFR as "Gold Standard"--All that Glitters Is Not Gold?". Clinical Journal of the American Society of Nephrology. 6 (8): 1813–1814. doi:10.2215/CJN.06040611. PMID 21784836.
^ "Chronic kidney disease in adults: assessment and management". NICE. Retrieved 19 August 2016.
^ abcd Guyton, Arthur; Hall, John (2006). "Chapter 26: Urine Formation by the Kidneys: I. Glomerular Filtration, Renal Blood Flow, and Their Control". In Gruliow, Rebecca. Textbook of Medical Physiology (Book) (11th ed.). Philadelphia, Pennsylvania: Elsevier Inc. pp. 308–325. ISBN 0-7216-0240-1.
^ abcd Keener, James; Sneyd, James (2004). "20: Renal Physiology". In Marsden, J.E. Mathematical Physiology (Book). Interdisciplinary Mathematics. Mathematical Biology Vol. 8. Sirovich, Wiggins (1st ed.). New York, NY: Springer Science +Business Media LLC. pp. 612–636. ISBN 0-387-98381-3.
^ "KDOQI CKD Guidelines". Archived from the original on 2012-10-03. Retrieved 2010-08-25.
^ GFR Calculator at cato.at – Cockcroft-Gault Archived 2004-09-05 at the Wayback Machine. – GFR calculation (Cockcroft-Gault formula)
^ Cockcroft DW, Gault MH (1976). "Prediction of creatinine clearance from serum creatinine". Nephron. 16 (1): 31–41. doi:10.1159/000180580. PMID 1244564.
^ Gault MH, Longerich LL, Harnett JD, Wesolowski C (1992). "Predicting glomerular function from adjusted serum creatinine". Nephron. 62 (3): 249–56. doi:10.1159/000187054. PMID 1436333.
^ ab Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D (March 1999). "A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of Diet in Renal Disease Study Group". Annals of Internal Medicine. 130 (6): 461–70. doi:10.7326/0003-4819-130-6-199903160-00002. PMID 10075613.
^ Mathew TH, Johnson DW, Jones GR (October 2007). "Chronic kidney disease and automatic reporting of estimated glomerular filtration rate: revised recommendations". The Medical Journal of Australia. 187 (8): 459–63. PMID 17937643.
^ Joint Specialty Committee on Renal Disease (June 2005). "Chronic kidney disease in adults: UK guidelines for identification, management and referral" (PDF). Archived from the original (PDF) on 2007-10-19.
^ Davey RX (January 2006). "Chronic kidney disease and automatic reporting of estimated glomerular filtration rate". The Medical Journal of Australia. 184 (1): 42–3, author reply 43. PMID 16398632.
^ Twomey PJ, Reynolds TM (November 2006). "The MDRD formula and validation". QJM. 99 (11): 804–5. doi:10.1093/qjmed/hcl108. PMID 17041249.
^ Kallner A, Ayling PA, Khatami Z (2008). "Does eGFR improve the diagnostic capability of S-Creatinine concentration results? A retrospective population based study". International Journal of Medical Sciences. 5 (1): 9–17. doi:10.7150/ijms.5.9. PMC 2204044. PMID 18219370.
^ National Kidney Foundation (February 2002). "K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification". American Journal of Kidney Diseases. 39 (2 Suppl 1): S1–266. doi:10.1016/S0272-6386(02)70081-4. PMID 11904577.
^ ab Rule AD, Larson TS, Bergstralh EJ, Slezak JM, Jacobsen SJ, Cosio FG (December 2004). "Using serum creatinine to estimate glomerular filtration rate: accuracy in good health and in chronic kidney disease". Annals of Internal Medicine. 141 (12): 929–37. doi:10.7326/0003-4819-141-12-200412210-00009. PMID 15611490.
^ Levey AS, Coresh J, Greene T, et al. (August 2006). "Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate". Annals of Internal Medicine. 145 (4): 247–54. doi:10.7326/0003-4819-145-4-200608150-00004. PMID 16908915.
^ "GFR MDRD Calculator for Adults". National Kidney Disease Education Program. United States: National Institutes of Health.
^ Hougardy, JM; Delanaye, P; Le Moine, A; Nortier, J (2014). "Estimation of the glomerular filtration rate in 2014 by tests and equations: strengths and weaknesses". Rev Med Brux. (in French). 35 (4): 250–7. PMID 25675627.
^ Levey AS, Stevens LA, Schmid CH, et al. (May 2009). "A new equation to estimate glomerular filtration rate". Annals of Internal Medicine. 150 (9): 604–12. doi:10.7326/0003-4819-150-9-200905050-00006. PMC 2763564. PMID 19414839.
^ Matsushita K, Selvin E, Bash LD, Astor BC, Coresh J (April 2010). "Risk implications of the new CKD Epidemiology Collaboration (CKD-EPI) equation compared with the MDRD Study equation for estimated GFR: the Atherosclerosis Risk in Communities (ARIC) Study". American Journal of Kidney Diseases. 55 (4): 648–59. doi:10.1053/j.ajkd.2009.12.016. PMC 2858455. PMID 20189275.
^ Saleem, Mohamed; Florkowski, Christopher M; George, Peter M (2008). "Comparison of the Mayo Clinic Quadratic Equation with the Modification of Diet in Renal Disease equation and radionuclide glomerular filtration rate in a clinical setting". Nephrology. 13 (8): 684–688. doi:10.1111/j.1440-1797.2008.01045.x. ISSN 1320-5358.
^ ab Fontsere, N.; Bonal, J.; Salinas, I.; de Arellano, M. R.; Rios, J.; Torres, F.; Sanmarti, A.; Romero, R. (2008). "Is the New Mayo Clinic Quadratic Equation Useful for the Estimation of Glomerular Filtration Rate in Type 2 Diabetic Patients?". Diabetes Care. 31 (12): 2265–2267. doi:10.2337/dc08-0958. ISSN 0149-5992. PMC 2584175. PMID 18835955.
^ ab Schwartz GJ, Haycock GB, Edelmann CM, Spitzer A (August 1976). "A simple estimate of glomerular filtration rate in children derived from body length and plasma creatinine". Pediatrics. 58 (2): 259–63. PMID 951142.
^ ab Schwartz GJ, Feld LG, Langford DJ (June 1984). "A simple estimate of glomerular filtration rate in full-term infants during the first year of life". The Journal of Pediatrics. 104 (6): 849–54. doi:10.1016/S0022-3476(84)80479-5. PMID 6726515.
^ Brion LP, Fleischman AR, McCarton C, Schwartz GJ (October 1986). "A simple estimate of glomerular filtration rate in low birth weight infants during the first year of life: noninvasive assessment of body composition and growth". The Journal of Pediatrics. 109 (4): 698–707. doi:10.1016/S0022-3476(86)80245-1. PMID 3761090.
^ Haenggi MH, Pelet J, Guignard JP (February 1999). "[Estimation of glomerular filtration rate by the formula GFR = K x T/Pc]". Archives de Pédiatrie (in French). 6 (2): 165–72. doi:10.1016/S0929-693X(99)80204-8. PMID 10079885.
^ Schwartz GJ, Muñoz A, Schneider MF, et al. (March 2009). "New equations to estimate GFR in children with CKD". Journal of the American Society of Nephrology. 20 (3): 629–37. doi:10.1681/ASN.2008030287. PMC 2653687. PMID 19158356.
^ Stevens LA, Coresh J, Schmid CH, et al. (March 2008). "Estimating GFR using serum cystatin C alone and in combination with serum creatinine: a pooled analysis of 3,418 individuals with CKD". American Journal of Kidney Diseases. 51 (3): 395–406. doi:10.1053/j.ajkd.2007.11.018. PMC 2390827. PMID 18295055.
^ abcd M Thorp (2004). "An Approach To The Evaluation Of An Elevated Serum Creatinine". The Internet Journal of Internal Medicine. 5 (2). doi:10.5580/1d4b.
^ Bauer C, Melamed ML, Hostetter TH (2008). "Staging of Chronic Kidney Disease: Time for a Course Correction". American Society of Nephrology. 19 (5): 844–46. doi:10.1681/ASN.2008010110.
^ Eckardt KU, Berns JS, Rocco MV, Kasiske BL (June 2009). "Definition and Classification of CKD: The Debate Should Be About Patient Prognosis—A Position Statement From KDOQI and KDIGO" (PDF). American Journal of Kidney Diseases. 53 (6): 915–920. doi:10.1053/j.ajkd.2009.04.001. PMID 19406541. Archived from the original (PDF) on 2011-07-25.
^ "KDIGO Controversies Conference: Definition, Classification and Prognosis in CKD, London, October 2009". Kidney Disease: Improving Global Outcomes (KDIGO). 2009. Archived from the original on 2010-11-24.
External links
Online calculators
- Online GFR Calculator
Schwartz formula for estimating pediatric renal function
Creatinine clearance calculator (Cockcroft-Gault Equation)- by MDCalc- MDRD GFR Equation
- GFR calculator using Cystatin C
Reference links
National Kidney Disease Education Program website. Includes professional references and GFR calculators- eGFR at Lab Tests Online


